BY Sam Moore
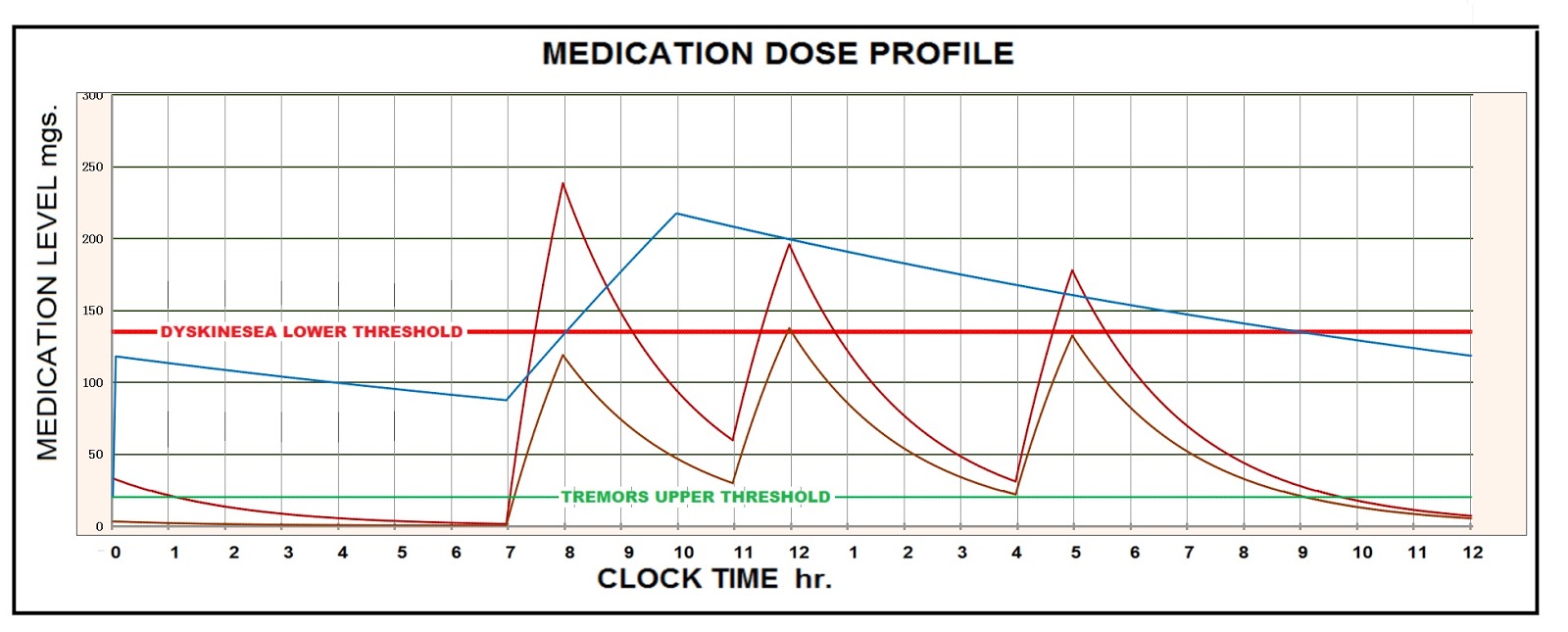
I have found that my dyskinesia has a susceptibility range. The range starts at about 100 mgs of levodopa IR and continues at levels of levodopa higher than I have experienced. The Figure below shows the range I have experienced. The intensity of the dyskinesea, when it occurs is proportional to the highest level just before the elimination period starts. At levels less than the susceptible range is a safe range. This range starts at a level where the tremors cease.
The information is patient sensitive and will not be the same for everyone. Relating the information to blood concentration, one hundred mgs. is equivalent to approximately 18.2 mg/ml blood concentration. For my body weight, about 5.5 liters of blood.
The blue/green line is for 150 milligrams taken three times a day. While I was on that protocol I did not suffer with tremors or dyscinesea. I attribute that to the level being most of the time above the upper limit of tremors. I believe this dose level is too low to be therapeutically beneficial.
The red line is for 200 mg. taken 4 times a day. This was the worst I have suffered with dykinesea, both in length and intensity. I never want to go through that again. The higher the peak just before the dyskinesea, the higher the intensity.
I have been looking at profiles of Rytary. I think I have it down pretty good. I understand that a friend of mine is taking Rytary, Two 95 mg. tablets, 4 times a day. I worked up a model of Rytary so I could plot a graph of the daily profile. The result is the graph, shown below.
.
From my experience, I have found that you can have a condition where you get enough levodopa to eliminate the tremors, without having enough to be therapeutic. If I am correct, in the protocol that my friend is on, I believe she is at this point. I have taken into account that she is a small woman and would not require as large a dose as a man my size. I believe in order to have a therapeutic effect you must have enough levodopa to make you susceptible to dyskinesea. Fortunately, with the Rytary protocol, the level of medication remains at a high enough level to prevent triggering of dyskinesea. In the plots, I have shown the profile for the 190 mg. tablet.

I am impressed by the Rytary profile, because you can get 24 hour coverage and it is less susceptible to Dyskinesea than my current protocol. Except for the cost, I think Rytary is the best solution yet for a sinemet protocol.
I believe that for ease in comparing results between patients, it makes more sense to look at the profiles in terms of mg/ml, rather than in mgs. Mgs/ml takes into account the weight of the patient with there associated blood volume. In order to support this recommendation I have attached a graph with two profiles. One is of two 95 mg. tablets of Rytary taken 4 times a day by a 155 lb. patient. he other graph is of two 95 mg. tablets of Rytary taken 4 times a day by a 110 lb. patient.
I believe that for ease in comparing results between patients, it makes more sense to look at the profiles in terms of mg/ml, rather than in ml. This takes into account the weight of the patient with the associated blood volume. In order to support this recommendation I have attached a graph with two profiles. One is of two 95 mg. tablets of Rytary taken 4 times a day by a 155 lb. patient. The other graph is of two 95 mg. tablets of Rytary taken 4 times a day by a 110 lb. patient.

As can be seen in the graphs, the dose has a much stronger effect on the smaller patient. This technique will narrow the gap for comparing results.
I hope you have found this article beneficial. If so, please "Like" it on Facebook, or comment on my blog. Support PD research on the Michael J. Fox foundation. Support this blog with donations to my account s_durwood_m@msn.com on Paypal, or contact sdurwoodm@gmail.com to send comments. Both positive and negative comments are welcome, although positive ones are preferred. I will try to respond.
No comments:
Post a Comment