HOW DO YOU EVICT SQUATTERS?
This is a story about troubles with the Parkinson’s clan.
I have a problem with squatters that have moved in and won’t go away. It started out innocently enough. It would be a situation that was unpleasant but tolerable. It began about six years ago when the patriarch of the family moved in. The family name is Parkinson.
Soon other members of the family showed up. There were Tremor, Stiffness, Lethargy, Insomnia and several others that moved in and out.
It soon became intolerable. I started looking for someone to help me get rid of the unwanted visitors. I selected a specialist with important letters before and after her name, only to be informed that she had no solution for my problem. I then found another specialist, again with impressive credentials. He started out trying several approaches. Some of the approaches did no more than temporally move some of the family out but they always returned. He tried one approach that involved the marriage of the patriarch to Levo. At this point, the marriage produced an unplanned son that was named Dyskinesea. Dyskinesea was too much for the specialist so he recommended another specialist that had narrowed his specialty to the Parkinson’s family.
The new specialist was sold on the marriage of the patriarch to Levo. He tried marriage counselling to increase the bond between the two. This worked to some extent; however, the relationship had lots of ups and downs. Part of the problem with the marriage was Levo's chronic gastric problem. The solution to the problem was getting Carbi involved. Carbi and Levo were twins of the Dopa family, and had been separated by the marriage.
At this point in time the relationships were complicated by an across the country move. I moved to live with my daughter and her family. She fixed up a nice apartment for my wife and me in her home.
A perfect opportunity to get away from the Parkinson’s clan. Think again, they found a sucker and they intend to milk it dry. So now I have to start again. First find a new specialist. My fourth specialist was there in name only. I think he had retired early and forgot to tell anyone.
So the patriarch followed with his clan and his wife, Levo, and moved in on us again.
I was getting desperate at this stage, so I decided to foster a romance between Dyskinesea and a new entry, Mary Jane. Mary Jane became an option because she was living in the state of California, where we had moved. This was a failure, so I continued my search for a new specialist. Enter number five.
Like number four, number five had also entered premature retirement.. At this stage I gave up and decided I would have to go proactive. I started by going to the internet and researching the various aspects of the Parkinson’s clan.
I discovered that the Dopa family was extremely sensitive to the timing of their involvement. I used a timer to time my attempts at involving Levo in the relationship. An immediate improvement resulted. Then I found that a greater improvement occurred when I adjusted the intensity of my attempts. By adjusting the intensity of the attempts along with the timing of the attempts, I could get an amplification of the effect.
Something was still missing. I had no way of correlating the intensity and timing with the timing of the response from Levo. Then I found that others had measured the push back response of Levo. I could then predict the action of Levo by plotting the intensity of the attempt against timing of the attempts. At first I manually plotted the chart using “Paint” and the laws of geometry. This was slow and tedious, but it was an improvement in performance. I then went to the computer and developed a spreadsheet algorythm to have the computer generate and plot the data for me.
I tried to interest my fifth specialist in my discovery, but he didn’t want to be bothered with any new ideas. I found a sixth specialist. Number six was a jackpot. He was interested in my approach and encouraged me to continue developing the algorythm.
Number six decided that arbitration was in order, so he brought in two negotiators to try to bring some peace to the family. He decided on Amanta and Rogeta, two intercessors who were able to smooth over some of the rough spots in the inter-family relationships. Getting the arbitration process going had its own rough spots due to the high cost of the Rogeta half of the team. Negotiating the contract price was difficult in itself.
That brings the story up to date. I still have the clan on my back, but it is more predictable. My next effort is to help others who have the same problem as I have.
If any reader of this story has any ideas about this subject, please contact Sam at sdurwoodm@gmail.com.
“HOW DO YOU EVICT SQUATTERS?” EXPLAINED
The short story “HOW DO YOU EVICT SQUATTERS?” was written to put some humor into the other wise hum drum life of PD patients. For most patients the story would make sense; however, for the person unfamilier with the levodopa treatment of PD, some of the situations of the story might not be clear. I will attempt to give some baqckground on the most prevalent treatment of the disease.
First PD is a progressive disease. As of this date, it is incurable. The best that can be done is minimize the symptoms of the disease. It is believed that either a deficiency of Dopamine or a defect in the ability of the brain to utilize the Dopamine for firing the syenapsis. The inability of the brain to utilize Dopamine, causes erratic firing of the synapses, resulting in erratic responses in the movement of the patient and slowness of movement with sometime freezing of motion. This symptom of PD is called Tremors. Years ago, it was discovered that the medication, levodopa minimizes the symptom, dyskinesea, as well as the other symptoms that tended to immobilize the patient.
The problem this treatment has severe side effects of its own. By adding carbidopa to the dose, the symptom nausea is minimized. The medication, brand name Sinemet, provides a 1:4 ratio mixture of carbidopa and levodopa. This is available in a generic version with a number of absorption characteristics, Imediate Release, Control Release, Extended Release, and combinations of the three such as Rytary.
The biggest drawback to levodopa is its short half life. The half life is approximately 1.5 hours. This means that 1/2 the levodopa is eliminated within 1.5 hours. In addition, the levodopa is a precursor to Dopamine. The levodopa does not cross the blood/brain cell barrier, resulting in the requirement of a massive amount of levodopa being required to provide adequate dopamine. Most of the levodopa is eliminated and never reaches the barrier.
Combinations of the available characteristics are used to extend the length of time a therapeutic dose stays in the blood stream. I work with the total medication in the blood stream for my profiles, A simple conversion multiplier will change the total medication level, in milligrams to blood concentration, in milligrams/milliliter. The only added information required is the weight of the patient.
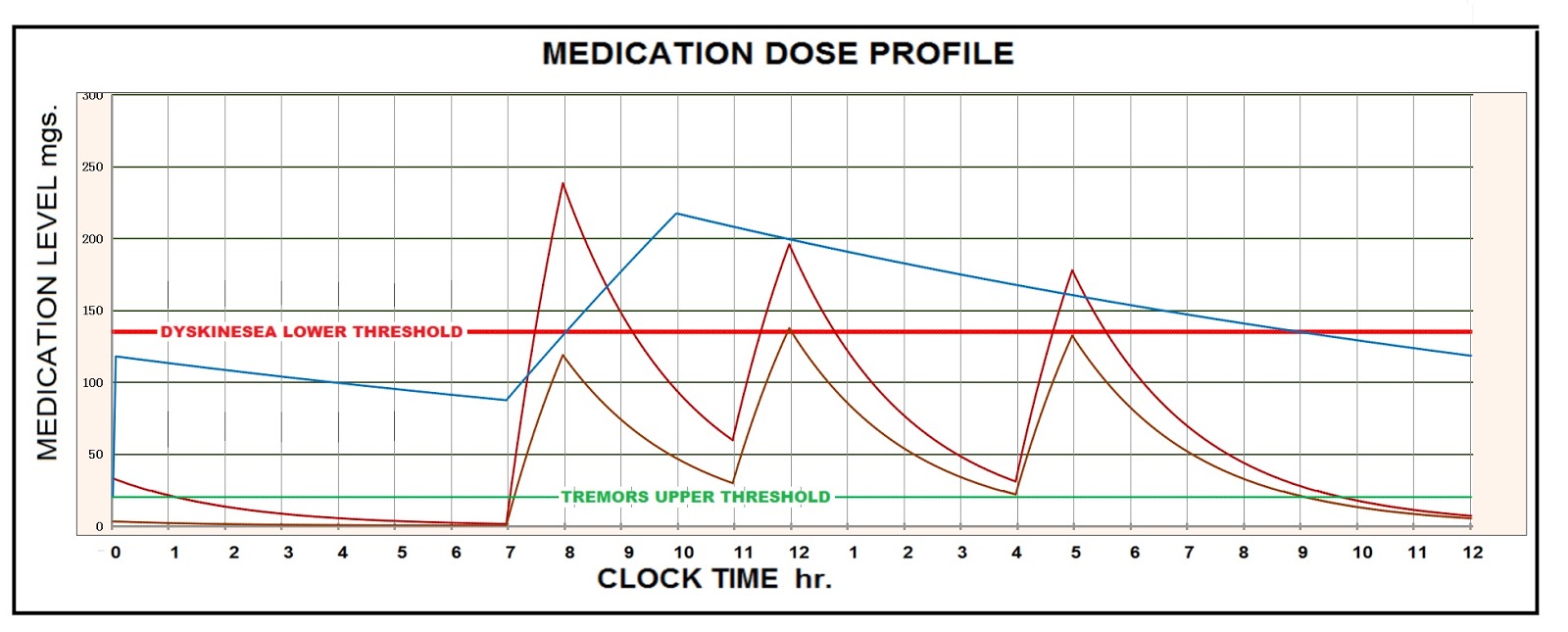
A plot of blood content of levodopa vs time of day gives the “Profile” of the day’s medication protocol. This is a valuable tool in fine tuning the protocol for optimum results. Even with the Profile optimized, the protocol is limited in its effectivity.
With the goal of supplementing the supply of dopamine another approach was desired. A search for a supplement to dopamine resulted in some agonist candidates. Two such agonist were found, Amantadine and Rotegotine. Amantadine has been used for several years to relieve the dyskinesea created by a drop in the levodopa level. It is available in a generic form. It has an absorption time of approximately 3 hours and an elimination half life of approximately 16 hours. Since the medication half life is long. the medication blood level remains relatively high throughout the day. Unlike levodopa, the medication crosses the blood/brain barrier. I assume that the Amantadine has a chemical change in crossing the barrier. The resulting agonist supplements the dopamine. A relatively large dose is required to force the medication across the barrier. The original use for Amantadine was as a deterant to some kinds of pneumonia.
On the other hand the Rotigotine, is only available as a brand name medication, Neupro Patch. The manufacturer selected a derma patch as the delivery system. Without financial help, I cannot afford the medication. The patch is changed every 24 hours. In the 24 hour period It delivers 45% of the total medication in the patch. I have been unable to profile the patch. The modeling is complicated by the dual and relatively short half life combined by the characteristics of the delivery system. I believe the total blood stream level, after several days stabilization, is considerably less than the medication delivered in the 24 hours. Due to the high cost of the medication, some patients have resorted to wearing the patch for 48 hours, thus halving the cost. I would not recommend that action even though 65% of the medication remains in the patch after 24 hours. My intuition tells me the variation of medication level would cause an increase in the susceptibility to dyskinesea.
“Mary Jane” refers to my experimenting with PD’s response to medical marijuana. I know of one case where medical marijuana has extended the quality life span of a cancer patient by several years. THC is the ingredient in cannabis that is said to reduce the symptoms of PD and Dyskinesea. It didn’t work for me but that doesn’t say it won’t work for others. Another successful case for cannabis was for alleviating the withdrawal symptoms from opioids. The patient had used opioids for several years for pain relief. When his pain went away he was unable to withdraw from the opioids because of sleeplessness and other severe symptoms. With the cannabis he was able to overcome the addiction.
If you found this blog beneficial donate to PD research with The Michael J. Fox Foundation. Send your Likes or Dislikes to Sam at sdurwoodm@gmail.com. You can support this blog through donations through PayPal for sdurwoodm@gmail.com.